Deciphering How NLRP3 Incites the Stromal Response in Kawasaki Vasculitis
Abstract
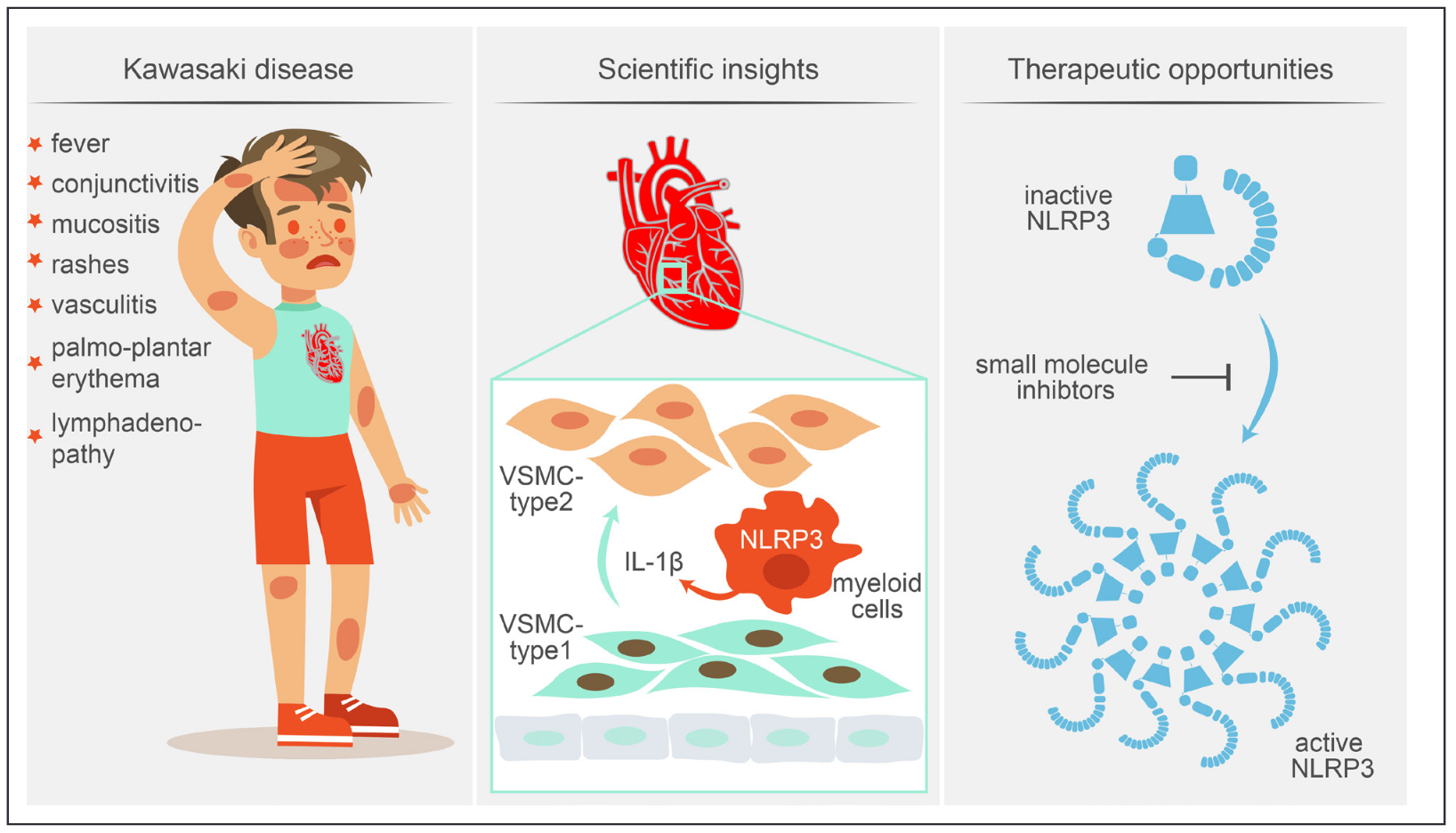
Kawasaki disease (KD), also known as Kawasaki syn-drome, is one of the most common acute vasculitides in children. KD is typically a febrile self-limited illness that, if untreated, can lead to coronary artery aneurysms that can ultimately result in accelerated atherosclerosis, myocardial infarction, and resultant heart failure. The disease, described initially by Tomisaku Kawasaki in the 1960s1,2 is clinically accompanied by fever lasting >5 days and signs of mucocutaneous inflammation. These physical findings, which often do not appear simultane-ously, include bilateral nonexudative conjunctivitis, rashes, mucositis, cervical lymphadenopathy, and changes at the extremities, such as palmar or plantar erythema. In about 40% of children with KD, a concurrent infection can be diagnosed at the clinical presentation, which makes determining the cause of fever particularly challenging.
Read more at Circulation Research